MAY 8, 2026 – In continuation of the pursuit of continuing legal education (“CLE”) credits, I’m in the middle of a six-hour webinar symposium on “Universal and Quality Health Care,” sponsored by the University of St. Thomas School of Law (St. Paul, MN). Again, along with a host of UST-sponsored CLE courses on constitutional law in the Age of Trump, this one is a doozy.
One drawback to the Age of Information is an over-abundance of “it,” of information. To characterize this as a “drawback” is strikingly counter-intuitive. In addressing any major societal challenge, isn’t more information desirable—as long as the information is factually trustworthy? The downside, however, isn’t the quantity of tested, vetted, scrutinized, data-supported information. It’s our limited cerebral capacity, at the individual voter level, to absorb, synthesize and analyze it to a point of refinement sufficient to guide ballot decisions—assuming, of course, that we still live in an effective representative democracy.
This lack of capacity is currently driven by three factors: 1. The crushing demands on our time and attention regarding personal, familial, social and vocational affairs, each inundated with . . . information transmitted by multiple means; 2. The complexity of a fast-evolving world of eight billion people interacting on multiple levels, economically, politically, and socially—particularly against a backdrop of perpetual strife and competition over access to scarce and shared resources; and 3. The unnecessary chaos created by a single powerful individual and his all too numerous surrogates, stoked by an uninterrupted cycle of memes and outbursts filling our smartphone screens and speakers, often with disinformation and misinformation.
Our limited capacity for managing information walks hand-in-hand with a narrowing of attention spans. We’ve been trained and lulled into surrendering our power of concentration on any one thing for more than mere minutes. Memory, a facet of concentration, has become largely obsolete in a world dominated by apps and increasingly, by AI. Need to “figure out” the solution to a problem? No you don’t:“Go Google . . . and leave the searching to us.”[1]
In this brave new world of uninterrupted information flow, we find ourselves drowning in data, desperately trying to keep our nostrils above the waterline so that we can manage our lives from one day to the next. This being our condition, what time and space is reserved for learning about, understanding, then making informed decisions about the big whopping issues looming over the whole of society—matters critical to our health, wealth, and happiness?
Such as . . . health care in America, for instance—the subject of that webinar I mentioned at the outset of this post.
If now I’m not leading a life half as frenetic as I did 10, 20 or 30 years ago, or a tenth as crazy as the life that people around me seemed to have led, I’m still busy enough not to be taking deep dives into the imponderable issues—such as health care in America. Only by necessity of gathering CLE credits did I find myself in the very deep end of the pool of perennial national problems. Energy, which I addressed in a post last week, is another issue at the deep end of the pool. Education is yet another. And of course, deep down in the fathomless end of the pool is our broken political system—and obsolete constitution framework.
But back to health care in America. As residents of the Twin Cities, my wife and I have access to some of the best medical care in the world. As Medicare beneficiaries with supplemental Advantage Plan policies, my wife and I have excellent health insurance—which wasn’t the case prior to our eligibility for Medicare. But the not-so-good coverage coincided with low-intensity medical care needs. In any case, that was then, and our “great” insurance is now—along with high-end medical needs—thus minimizing our exposure to the considerable material flaws in the American medical insurance model. Accordingly, I’d never had much of a personal incentive to study the present system with the aim of developing informed opinions about it and the various the various proposed reforms.
Three hours (so far) of the CLE webinar have served as the equivalent of being tossed into the “deep end of the pool,” at least as it relates to the imponderable challenges of health care and insurance in America. The presenters are an impressive panel of experts; people who’ve done extensive research, who know the intricacies of the jungle of laws and regulations pertaining to health care coverage, and who’ve applied major analyses to what is an infinitely complex part of our lives and economy. I heard impassioned arguments for a “single payer” model of health insurance and listened to equally serious challenges to such a system—delivered not by private industry representatives whose oxen would be gored by a single payer system but by academics who’ve gathered and analyzed mountains of pertinent and rigorously tested . . . information.
I’m now no closer to being an “expert” than I was before hearing bona fide experts, but I’ve thus far become more aware of several critical aspects of the overall issue of health care in America.
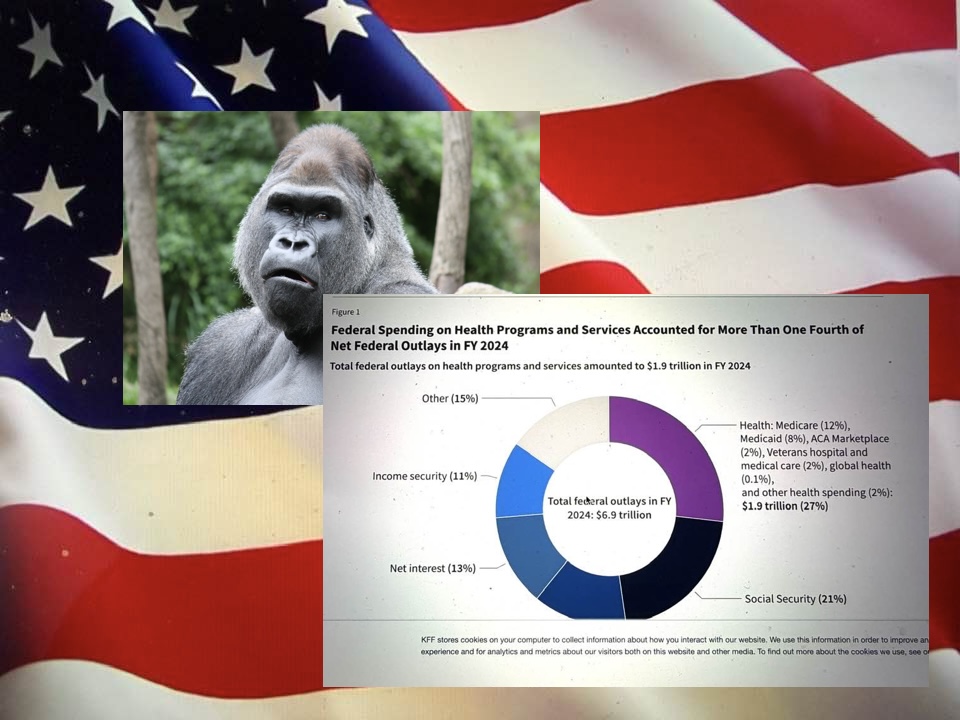
First, for a frame of reference, is the economic significance of health care: over 18% of GDP and growing; 27% to 29% of the federal budget. A meaningful reduction in federal spending (and corresponding reduction of the worrisome federal deficit) simply cannot be achieved without reining in expenditures on health care; it’s a matter of simple math.
Second, especially with an aging population, the cost and quality of health care will loom larger among our “needs” and “wants.” Inject another Covid-19-like health crisis into the picture, and the system will be stressed beyond its limits, producing an array of sub-crises from financial and economic to social and political.
Third, as the webinar experts themselves conceded, no “perfect,” let alone “simple” solutions exist for what most people would agree in principle are the two essentials of health care: (a) access; and (b) affordability. Significant discussion concerned the conundra of statutory, regulatory and administrative definitions. For example, what is meant, exactly, by the phrase “universal health care,” “affordable health care” and “quality health care”—in a world of finite resources? Politically, how do policy makers achieve broad buy-in to health care reforms, when the vast majority of voters support “universal health care” but overwhelmingly oppose having to pay for it? The existing system “works” fine for people such as my wife and me, but it’s utterly broken for so many other sectors of society. Worse yet, some of the “broken” aspects are self-perpetuating. For example, to qualify for Medicaid, recipients must be “poor,” but if they seek not to be “poor” (or alternatively, not “as poor”), they’d no longer qualify for Medicaid[2]—and yet not have access to an affordable alternative; given their health care needs and financial limitations (continuing above the official poverty level), their most rational choice is to remain irrationally “poor.”
I have three hours of the webinar to go and am curious (and worried) about what additional troubled ground will be explored. Thus far, I have three overarching and related reactions: 1. Substantial reform of our health care system is essential; 2. I’m thankful that our society has produced people willing to devote their entire professional lives and energies to a deep study of the system and generation of ideas for reform; and 3. What should upset us most about the clown show in the White House 16 months into the circus is the gross malfeasance of leadership regarding the monumentally complex issue of health care in America. Just think about that the next time you hear about voter suppression efforts, redistricting shenanigans, ICE arrests and deportations, the billion-dollar ballroom, the triumphal arch, the gold-plated statue, the Big Beautiful Bill, use of DOJ investigations and indictments to punish political enemies, the Epstein Files, drastic budgetary and personnel cuts to the CDC, evisceration of environmental protections, runaway grift and corruption by the Trump family and billionaire friends or . . . ready for it? . . . the Strait of Hormuz and the price of gas.[3]
Subscribe to this blog and received notifications of new posts by email.
© 2026 by Eric Nilsson
[1] A throwback to the Greyhound Bus Lines slogan slapped on the sides of every bus, “Go Greyhound . . . and leave the driving to us.”
[2] The rules vary by state, some being more enlightened (and financially able) than others.
[3]Almost completely out of sight/out of mind: Ukraine. Completely off today’s radar: Venezuela.